frozen shoulder radiofrequency treatment
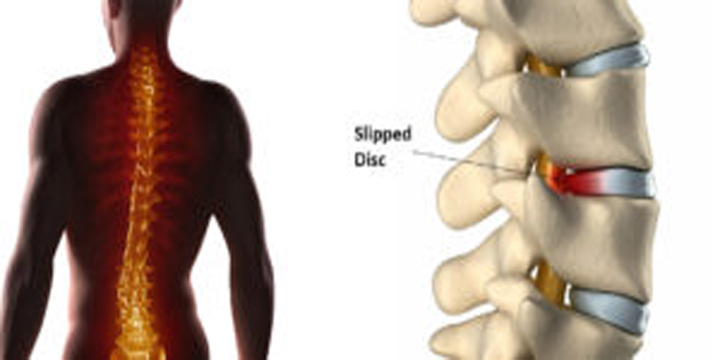
Shoulder pain
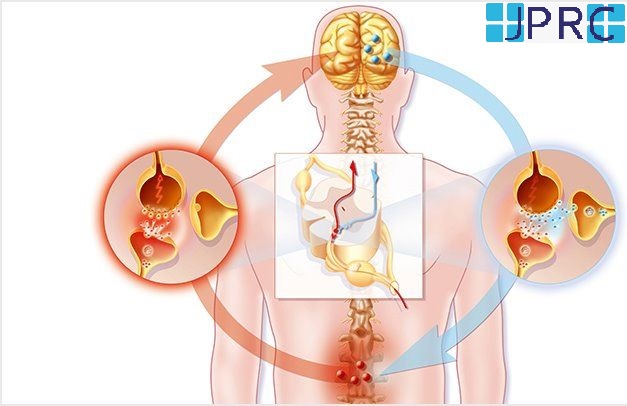
Shoulder pain is the second most common musculoskeletal disorder in adults over their lifetime. Shoulder disorders are often accompanied by acute, sub-acute, or chronic pain, and limited range of motion (ROM) Limited ROM of the shoulder joint affects upper extremity joint function and quality of life. Effective management of shoulder pain demands a multidirectional approach including medication, physical therapy, rehabilitation, surgical procedures, and selective nerve block for local pain management and Reduction of painful protective muscle spasms and modulation of afferent input and motor control may be facilitated by suprascapular nerve blockade. If the short-term effect of peripheral nerve block using local anaesthetics is not sufficient, other techniques may be used for long-term pain relief. Several case studies have reported a favourable outcome for pulsed radiofrequency (PRF) Neuromodulation to the suprascapular nerve (SSN)
Suprascapular pulse RF technique
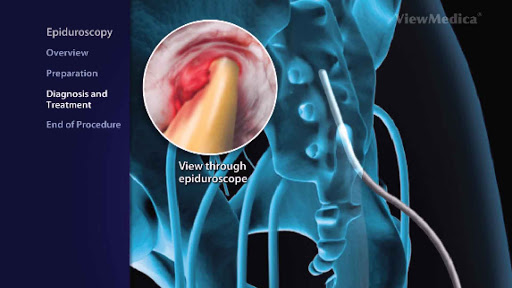
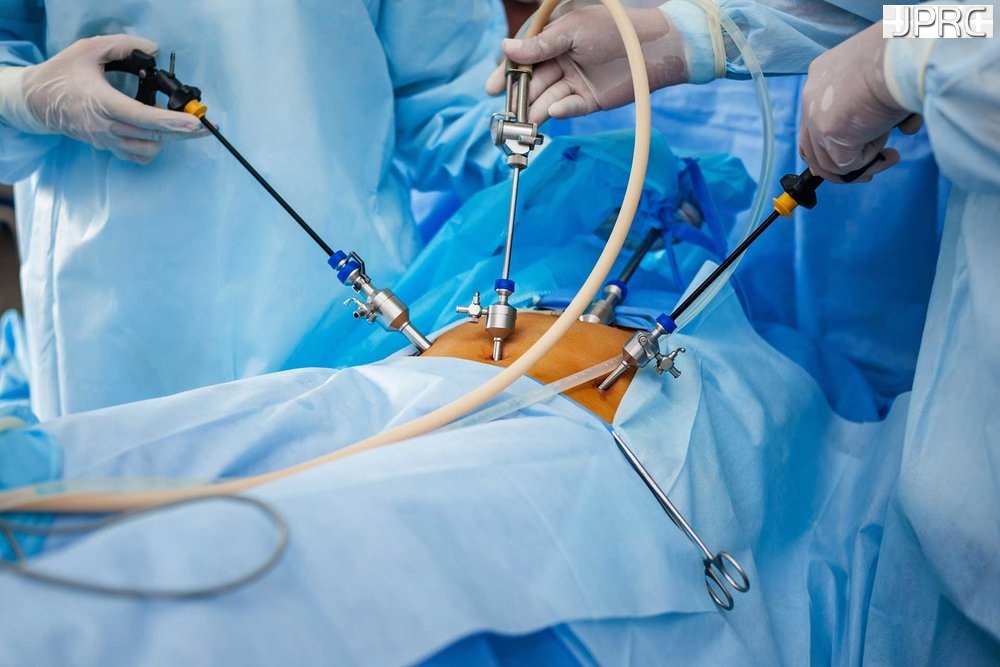
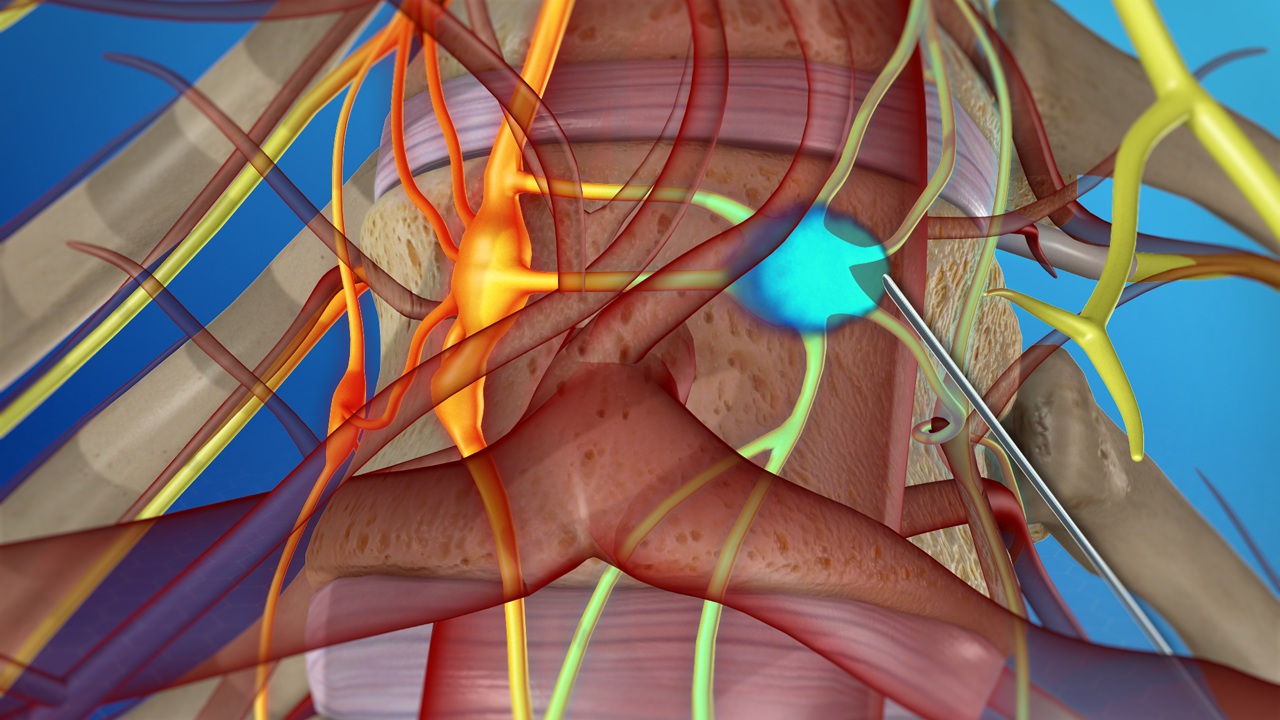
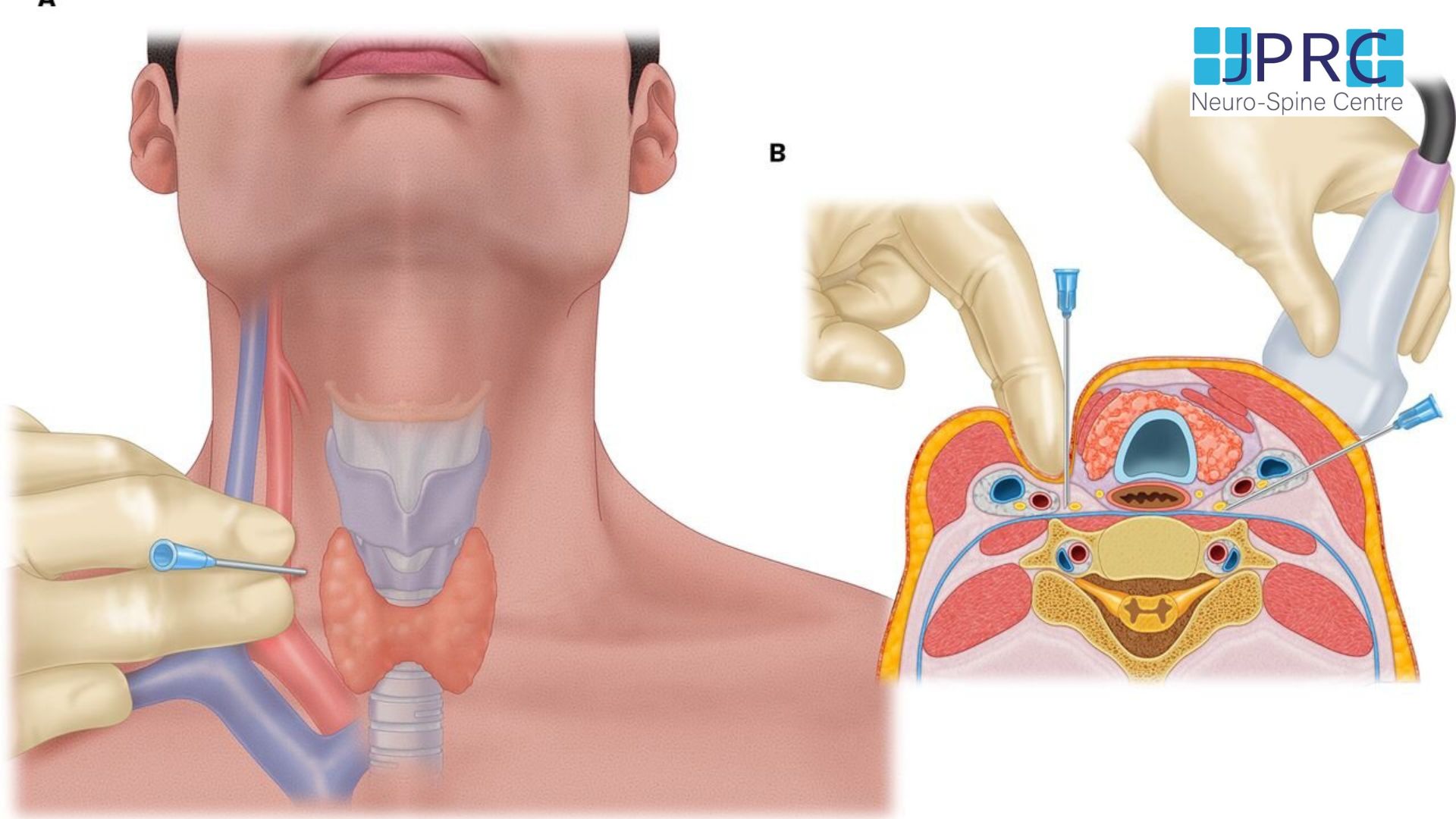
The PRF procedure was performed in the operating room under fluoroscopy using a radiofrequency generator. The C-arm was oblique about 10-20° and angled cephalo-caudad about 10-20°. The suprascapular notch was easily identified as superior to the scapular spine, medial to the coracoids process, and lateral to the rib margins.
The scapula area was clean with antiseptic betadine and draped with sterile towels. The skin was anaesthetized with 5% lidocaine gel. The spine of the scapula was located, and a line was drawn along it from the tip of the acromion to the medial scapular border. The midpoint of the line was determined and a vertical line parallel to the spine of the vertebral column was drawn through it. The angle of the upper outer quadrant was bisected with a line, and an X was marked on the line 1 cm from the apex of this angle A disposable 22-gauge, 15-cm Radiofrequency cannula with a 5-mm active tip was inserted at this point perpendicular to the skin in all planes. The author confirmed the correct needle tip relative to the suprascapular notch by fluoroscopic images. The introducer needle was withdrawn and the disposable RF electrode was advanced. Sensory stimulation (50 Hz) was performed after the needle tip penetrated the suprascapular notch. Sensory stimulation at 50 Hz was performed and reproducible paresthesias in the shoulder joint occurred at a voltage ≤of 0.3 V. Motor stimulation at 2 Hz was performed and contractions of the infraspinatus and supraspinatus muscles occurred at 0.4 V. After positive stimulation, PRF neuromodulation was performed for a total of 240 pulses at 50 V during which the temperature at the needle tip was not permitted to exceed 42℃.after that cannula removed and entry point close by adhesive tape and patient discharge after one-hour observation.
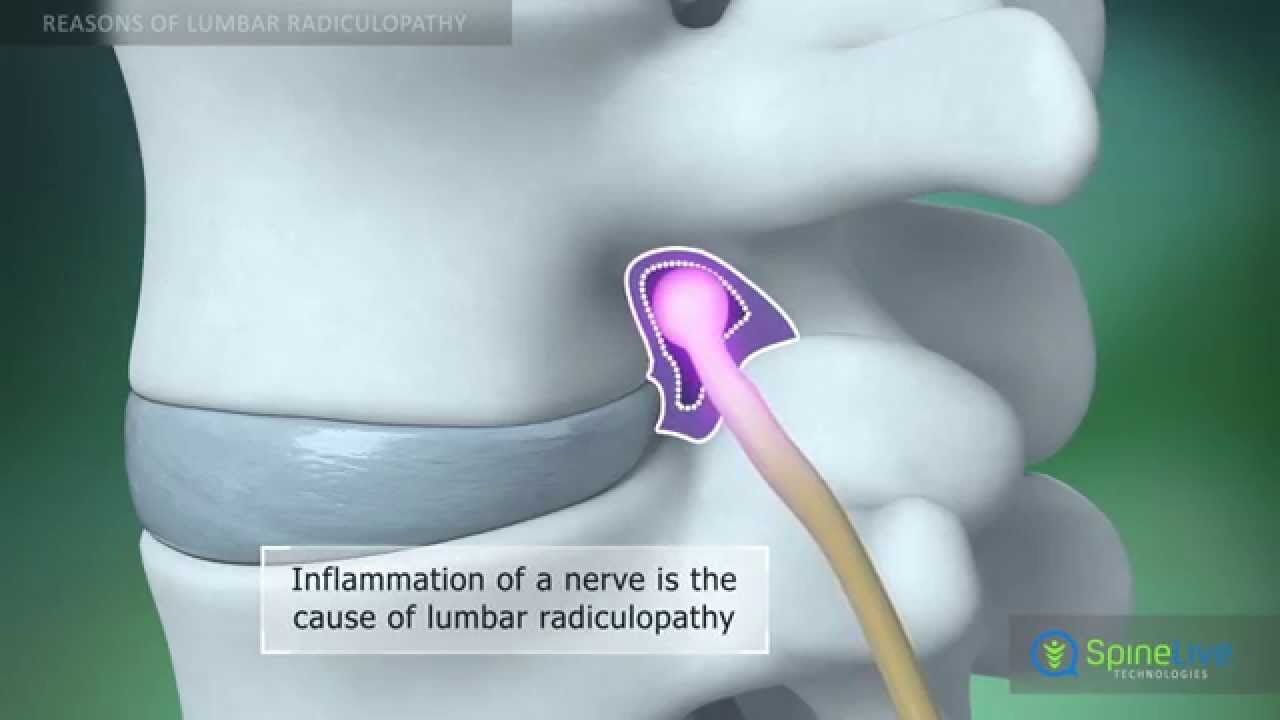
Clinical observation
The SSN has become a target for pain intervention because of its extensive sensory nerve supply to the shoulder structures, including the posterior glenohumeral joint capsule, acromioclavicular joint, subacromial bursa, and coracoclavicular ligament SSNB has been investigated in various types of chronic shoulder pain disorders Moreover, SSNB has a long history of reducing pain and improving Range Of Motion in patients with shoulder pain including rotator cuff lesions and frozen shoulder.


















































.jpg)










_Injection_Description_in_Hindi.jpg)














.jpg)









.jpg)




.jpg)
.jpg)
.jpg)






.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)








1.jpg)
1.jpg)
1.jpg)
1.jpg)
1.jpg)
1.jpg)
1.jpg)









2.jpg)
3.jpg)



4.jpg)
1.jpg)
2.jpg)

5.jpg)

6.jpg)


7.jpg)
2.jpg)

8.jpg)

9.jpg)
3.jpg)

10.jpg)

11.jpg)


12.jpg)
4.jpg)